Chapter 30 Tar - 1
Anti-inflammatory Effect of Glyteer
By K Takeuchi et al. (Fujinaga Pharm Research Division) published in the Journal of Pharmacological Sciences, 95(4) : 149-157, 1990.
Glyteer is a kind of tar (distilled liquid: black or brown viscous fluid gained by thermally decomposing organic matter) that has anti-itch/inflammation effects and has been used to treat dermatitis for a long time. (According to Fujinaga Pharm Co. documentation. It was released in 1924.)
Tar agents include coal tar, wood tar and ichthammol ointments. Coal tar and ichthammol ointments are popular as cheap over the counter drugs available without prescription.
When I was still working for the national hospital, an Australian woman came and asked me, “I need coal tar ointment for my child who has mild AD symptom. I don’t need potent drugs such as steroids. Any pharmacy in Australia sells coal tar, but I can’t find it in Japan. Where should I go to buy it?”
Medicines, having been applied since long time ago, with known effects and reasonable prices are rarely chosen as a subject of medical or pharmaceutical study.
When I began to work as a resident at the dermatological department in 1986, a sales person from Fujinaga Pharm, which I guess were not tied up with large pharmaceutical companies, complained that he had to take care of Tokai-Hokuriku region (central part of Japan consisting of 8 prefectures) alone. I remember hearing one doctor say laughing at him, “Dexamethasone with such a strong smell is out of date. Who will use glyteer now that steroids which are potent and convenient to use are released one after another?”
The paper introduced here was submitted by Hujinaga’s research division around that time. Maybe they wanted dermatologists to review the advantages of tar by pharmacologically verifying its effects.
Being written in Japanese, this paper provides precious data, for there are few that cover pharmacological action of topical tar drugs. Production of most topical tar drugs has been discontinued in Japan. Maybe they are too cheap to gain profit.
The paper compares the effects of glyteer, non-steroidal anti-inflammation agent and steroid agent for each experimental system according to Coombs and Gell allergy type classifications (I to IV).
The allergy can be classified into the following 4 types.
Classification of Allergy
Anti-inflammatory Effect of Glyteer
By K Takeuchi et al. (Fujinaga Pharm Research Division) published in the Journal of Pharmacological Sciences, 95(4) : 149-157, 1990.
Glyteer is a kind of tar (distilled liquid: black or brown viscous fluid gained by thermally decomposing organic matter) that has anti-itch/inflammation effects and has been used to treat dermatitis for a long time. (According to Fujinaga Pharm Co. documentation. It was released in 1924.)
Tar agents include coal tar, wood tar and ichthammol ointments. Coal tar and ichthammol ointments are popular as cheap over the counter drugs available without prescription.
When I was still working for the national hospital, an Australian woman came and asked me, “I need coal tar ointment for my child who has mild AD symptom. I don’t need potent drugs such as steroids. Any pharmacy in Australia sells coal tar, but I can’t find it in Japan. Where should I go to buy it?”
Medicines, having been applied since long time ago, with known effects and reasonable prices are rarely chosen as a subject of medical or pharmaceutical study.
When I began to work as a resident at the dermatological department in 1986, a sales person from Fujinaga Pharm, which I guess were not tied up with large pharmaceutical companies, complained that he had to take care of Tokai-Hokuriku region (central part of Japan consisting of 8 prefectures) alone. I remember hearing one doctor say laughing at him, “Dexamethasone with such a strong smell is out of date. Who will use glyteer now that steroids which are potent and convenient to use are released one after another?”
The paper introduced here was submitted by Hujinaga’s research division around that time. Maybe they wanted dermatologists to review the advantages of tar by pharmacologically verifying its effects.
Being written in Japanese, this paper provides precious data, for there are few that cover pharmacological action of topical tar drugs. Production of most topical tar drugs has been discontinued in Japan. Maybe they are too cheap to gain profit.
The paper compares the effects of glyteer, non-steroidal anti-inflammation agent and steroid agent for each experimental system according to Coombs and Gell allergy type classifications (I to IV).
The allergy can be classified into the following 4 types.
Classification of Allergy
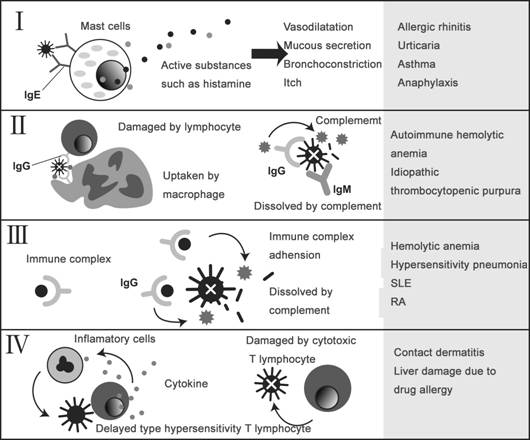
Type I is an immediate reaction type, Type II is an antibody-dependent hypersensitivity, Type III is a reaction caused by an immune complex of antigen and antibody, and Type IV is a delayed hypersensitivity (cell-mediated immune memory response).
Mice were used for each experimental system. As to type I, after intradermally injecting rat anti-ovalbumin serum (including immediate type anti-albumen IgE antibodies) into the mouse’s back, ovalbumin mixed with pigment (Evans Blue) was intravascularly injected. Measurement of Evans Blue contents in a given amount of cut off skin gets higher, as the immediate reaction becomes stronger and more pigment is leaked into the blood vessel. Effects on Type I depends on how much this pigment leakage can be contained by topically applied glyteer.
Mice were used for each experimental system. As to type I, after intradermally injecting rat anti-ovalbumin serum (including immediate type anti-albumen IgE antibodies) into the mouse’s back, ovalbumin mixed with pigment (Evans Blue) was intravascularly injected. Measurement of Evans Blue contents in a given amount of cut off skin gets higher, as the immediate reaction becomes stronger and more pigment is leaked into the blood vessel. Effects on Type I depends on how much this pigment leakage can be contained by topically applied glyteer.
** p<0.01(from the control) ## P<0.01(from the base)
Bufexamac and indomethacin are both non-steroidal anti-inflammation drugs (NSAID) and betamethasone 17-valerate is a steroid ointment.
For Type I, glyteer and steroid are effective, whereas NSAIDs are ineffective.
For Type I, glyteer and steroid are effective, whereas NSAIDs are ineffective.
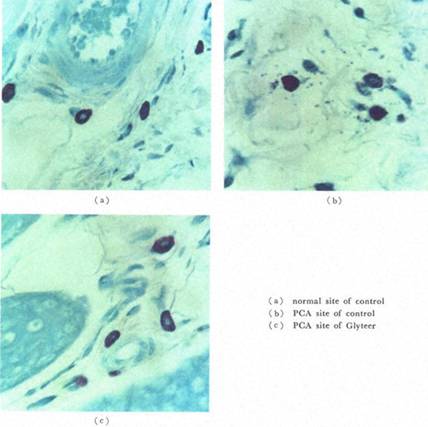
Shown above are pictures of murine skin tissue. Picture (a) is the image of a control specimen. Picture (b) shows Type I response where degranulated mast cells are releasing histamine. In Picture (c), degranulation is constrained because glyteer was topically applied in advance.
* p<0.05(from the control) # P<0.05(from the base)
As to Type II, glyteer is ineffective and steroid and NSAIDs are effective.
As to Type III, only steroid is effective and neither glyteer nor NSAIDs are effective
As to Type IV, all were effective in the order of steroid, glyteer and NSAIDs.
To summarize, glyteer was effective for Types I and IV, while NSAIDs were effective for Types II and IV. As far as Type IV is concerned, glyteer was more effective than NSAIDs. Steroid was effective for all types.
If I had seen these results in 1990, I should have had no interest and just thought, “Steroid is the most effective after all.”But I have different impression now that I know about addiction and rebound induced by long-term application of steroids. I’m pleased to know that glyteer is effective for Types I and IV, even though it is inferior to steroid. Actually, many doctors employ tar drugs in supporting steroid withdrawal.
Many doctors may wonder what they should use instead of steroids. Why not switching to new drugs such as Protopic (Tacrolimus) ointment or employing tar agents whose effectiveness and safety have been proved throughout the long history of its use.
Of course, there is a way to administer nothing if patients so desire, just keep an eye on them and support only when infectious disease or complications should develop. This is also a reliable medical practice for patients. What is required of doctors is not limited to prescribing drugs.
I’d like to say to dermatologists who have never treated patients addressing steroid withdrawal, “Why don’t you tell patients trying to stop all topical steroids without any drugs that you will administer no drugs, just monitor their conditions once a month and support them till they recover. Then you’ll become a reliable doctor for patients for the first time, not just a pharmacy.
To summarize, glyteer was effective for Types I and IV, while NSAIDs were effective for Types II and IV. As far as Type IV is concerned, glyteer was more effective than NSAIDs. Steroid was effective for all types.
If I had seen these results in 1990, I should have had no interest and just thought, “Steroid is the most effective after all.”But I have different impression now that I know about addiction and rebound induced by long-term application of steroids. I’m pleased to know that glyteer is effective for Types I and IV, even though it is inferior to steroid. Actually, many doctors employ tar drugs in supporting steroid withdrawal.
Many doctors may wonder what they should use instead of steroids. Why not switching to new drugs such as Protopic (Tacrolimus) ointment or employing tar agents whose effectiveness and safety have been proved throughout the long history of its use.
Of course, there is a way to administer nothing if patients so desire, just keep an eye on them and support only when infectious disease or complications should develop. This is also a reliable medical practice for patients. What is required of doctors is not limited to prescribing drugs.
I’d like to say to dermatologists who have never treated patients addressing steroid withdrawal, “Why don’t you tell patients trying to stop all topical steroids without any drugs that you will administer no drugs, just monitor their conditions once a month and support them till they recover. Then you’ll become a reliable doctor for patients for the first time, not just a pharmacy.

|

|
