Chapter 2 Epidermal Barrier Disruption Theory by Dr. Cork - 1
New perspectives on epidermal barrier dysfunction in atopic dermatitis: Gene–environment interactions
By MJ Cork et al. published in the J Allergy Clin Immunol Volume 118, Issue 1, Pages 3-21 (July 2006)
Since Dr. Kligman revealed the phenomenon of steroid addiction or flare rebound, this phenomenon has interested many clinicians and researchers.
The most persuasive theory to explain such phenomenon at present is the one presented by Dr. Cork in 2006 in the paper displayed above.
I’d like to provide the basic knowledge about skin structure for readers to understand his theory. Please look at the figure below.
New perspectives on epidermal barrier dysfunction in atopic dermatitis: Gene–environment interactions
By MJ Cork et al. published in the J Allergy Clin Immunol Volume 118, Issue 1, Pages 3-21 (July 2006)
Since Dr. Kligman revealed the phenomenon of steroid addiction or flare rebound, this phenomenon has interested many clinicians and researchers.
The most persuasive theory to explain such phenomenon at present is the one presented by Dr. Cork in 2006 in the paper displayed above.
I’d like to provide the basic knowledge about skin structure for readers to understand his theory. Please look at the figure below.
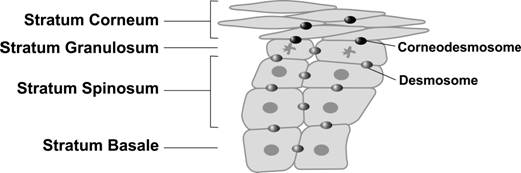
Epidermis is composed of the following 4 layers (from the deepest to the top): stratum basale, stratum spinosum, stratum granulosum and stratum corneum. Lower layer cells slowly differentiate into upper (outward) layer cells.
These cells are bound together by desmosomes and corneodesmosones to provide shield against environmental attacks. Corneocytes are bonded together by corneodesmosone.
These cells are bound together by desmosomes and corneodesmosones to provide shield against environmental attacks. Corneocytes are bonded together by corneodesmosone.
In the above illustration, you can see corneocytes are bonded together by corneodesmosome .
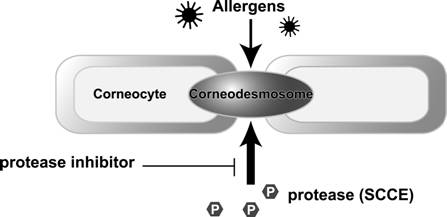
Corneocytes firmly locked together by corneodesmosomes make the stratum corneum, which functions as the barrier to protect the skin from allergens and other irritants. The structural integrity of the stratum corneum is maintained by enzymes called protease and protease inhibitor that are modulated in proper balance.
Proteases destroy corneodesmosomes to let old keratins naturally desquamate and inhibitors suppress such desquamation. As long as the balance between these substances are controlled properly, the stratum corneum keep proper thickness to protect the living body from allergens and other irritants.
Among several kinds of proteases, SCCE takes a major role. The SCCE is an endogenous protease derived from epidermal cells. Dr.Cork's claim is that prolonged application of topical steroids increases the protease and leads to breakdown of the epidermal barrier.
At the severe stage of atopic dermatitis (AD), inflammatory cell- or staphylococcus aureus-derived proteases are also active. As a result, integrity of the barrier function will be impaired, leading to allergen penetration.
Topical corticosteroids are effective to suppress severe skin inflammation, but long-term application makes the skin barrier impaired and vulnerable to allergen penetration, which is likely to cause AD aggravation.
Escalation of such condition into a vicious cycle, where flare can be cleared by TCS application but will get worse soon after TCS discontinuation, is called steroid addiction.
The below is the description of steroid addiction excerpted from Dr. Cork’s paper.
----- Excerpt -----
Topical corticosteroids are an important short-term treatment for severe flares of AD. However, if topical corticosteroids are used for prolonged periods and particularly on delicate skin sites, they can cause cutaneous atrophy and damage the stratum corneum. Prolonged use of topical corticosteroids might damage the skin barrier on delicate skin sites enough to enhance the penetration of irritants and allergens. This could provide the explanation for the phenomenon of posttopical steroid rebound and steroid addiction.
----- End of excerpt -----
Corneocytes firmly locked together by corneodesmosomes make the stratum corneum, which functions as the barrier to protect the skin from allergens and other irritants. The structural integrity of the stratum corneum is maintained by enzymes called protease and protease inhibitor that are modulated in proper balance.
Proteases destroy corneodesmosomes to let old keratins naturally desquamate and inhibitors suppress such desquamation. As long as the balance between these substances are controlled properly, the stratum corneum keep proper thickness to protect the living body from allergens and other irritants.
Among several kinds of proteases, SCCE takes a major role. The SCCE is an endogenous protease derived from epidermal cells. Dr.Cork's claim is that prolonged application of topical steroids increases the protease and leads to breakdown of the epidermal barrier.
At the severe stage of atopic dermatitis (AD), inflammatory cell- or staphylococcus aureus-derived proteases are also active. As a result, integrity of the barrier function will be impaired, leading to allergen penetration.
Topical corticosteroids are effective to suppress severe skin inflammation, but long-term application makes the skin barrier impaired and vulnerable to allergen penetration, which is likely to cause AD aggravation.
Escalation of such condition into a vicious cycle, where flare can be cleared by TCS application but will get worse soon after TCS discontinuation, is called steroid addiction.
The below is the description of steroid addiction excerpted from Dr. Cork’s paper.
----- Excerpt -----
Topical corticosteroids are an important short-term treatment for severe flares of AD. However, if topical corticosteroids are used for prolonged periods and particularly on delicate skin sites, they can cause cutaneous atrophy and damage the stratum corneum. Prolonged use of topical corticosteroids might damage the skin barrier on delicate skin sites enough to enhance the penetration of irritants and allergens. This could provide the explanation for the phenomenon of posttopical steroid rebound and steroid addiction.
----- End of excerpt -----

|

|
