Chapter 19 Involvement of Immune System
Corticosteroids Enhance the Capacity of Macrophages to Induce Th2 Cytokine Synthesis in CD41 Lymphocytes by Inhibiting IL-12 Production
By HD Rosemarie et al. published in the The Journal of Immunology, 1998, 160: 2231–2237
---- Excerpt -----
Although administration of corticosteroids may benefit acute asthma or allergic disease by directly inhibiting cytokine synthesis in T cells, enhanced production of Th2 cytokines by corticosteroid therapy may indirectly exacerbate allergic disease, which is caused by the overproduction of Th2 cytokines in allergen-specific CD41 T cells. This deleterious effect would result from a reduction in IL-12 synthesis by corticosteroids, thereby enhancing the production of Th2 cytokines, and limiting the production of Th1 cytokines.
----- End of excerpt -----
The author is a pediatrician (or rather a researcher) at Stanford University. Let me explain the key words first as the story about the immune system which tends to be complicated.
Corticosteroids Enhance the Capacity of Macrophages to Induce Th2 Cytokine Synthesis in CD41 Lymphocytes by Inhibiting IL-12 Production
By HD Rosemarie et al. published in the The Journal of Immunology, 1998, 160: 2231–2237
---- Excerpt -----
Although administration of corticosteroids may benefit acute asthma or allergic disease by directly inhibiting cytokine synthesis in T cells, enhanced production of Th2 cytokines by corticosteroid therapy may indirectly exacerbate allergic disease, which is caused by the overproduction of Th2 cytokines in allergen-specific CD41 T cells. This deleterious effect would result from a reduction in IL-12 synthesis by corticosteroids, thereby enhancing the production of Th2 cytokines, and limiting the production of Th1 cytokines.
----- End of excerpt -----
The author is a pediatrician (or rather a researcher) at Stanford University. Let me explain the key words first as the story about the immune system which tends to be complicated.
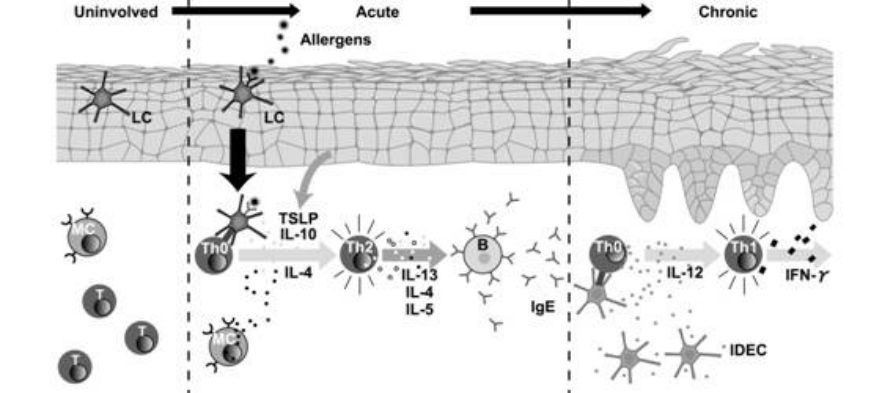
Each part divided by broken lines illustrates what is happening in the skin that is uninvolved, or affected by acute or chronic atopic dermatitis. At the acute phase, allergens induce IgE production by Th2 cells. At the chronic phase, IDEC (one of the antigen presenting cells) produces IL-12, making Th1 cells predominant.
Around 1998 when this paper was written, it was studied how steroids are involved in cytokine production in T cells. Researchers were interested in the strange phenomenon that steroids inhibit synthesis of most cytokines but increase Th2 cytokine, IL-4.
Dr. Rosemarie thought steroids may suppress the production of IL-12, which reduces IL-4 production, to increase IL-4, and proved it with experiments. The above excerpt was quoted from Discussion of her study. Making it simple, steroids seem to suppress inflammation in a short term but inhibit the transition from Th2 to Th1, possibly disturbing the natural healing mechanism.
However this remains controversial and a Swiss doctor expressed a different view in the paper on IL-12 in 2000.
Down-regulation of IL-12 by topical corticosteroids in chronic atopic dermatitis
By N Yawalkar etc. published in the J Allergy Clin Immunol Volume 106, Issue 5, Pages 941-947
He favors steroid application and writes that topical steroids inhibiting IL-12 synthesis prevent atopic dermatitis from proceeding to a chronic stage, where Th1 is predominant.
Such conflicting views come from a different perspective, considering the transition from Th2 (humoral immunity) to Th1 (cellular immunity) inflammation as the process of natural healing or that toward chronicity (obstinacy).
At any rate, Dr. Rosemarie’s concern about steroids that act to suppress IL-12 synthesis seems to have been forgotten since then.
Immune response is a chain of reactions and it is difficult judging whether a certain phenomenon is beneficial or not only by seeing a fraction of it. On the contrary, Dr. Cork’s barrier disruption theory is really clear and easy to understand.
Although the barrier disruption theory is prevalent as an explanation for steroid addiction or rebound, I think Dr. Rosemarie’s concern in 1998 is not groundless.
I have often seen IgE or eosinophil, a part of the immune system, remarkably increase in steroid addictive patients after withdrawal. It was not rare for IgE having kept normal value (within 500) to skyrocket to several tens of thousands or occasionally to hundreds of thousands, or for eosinophil to account for more than 50% of leukocytes in patients undergoing withdrawal (experiencing rebound). I think this phenomenon cannot be explained enough by vulnerability to allergen penetration based on Dr. Cork’s barrier disruption theory. ”Cytokine storm” of IgE or eosinophil version is happening. I think it is necessary to give supplemental explanation with the immune system involved.
The IgE and eosinophil levels, considered as AD severity markers, remain high for a while after steroid withdrawal and are not useful for judging flare conditions. They will go down only when steroids are administered again, which does not mean remission at all. As the rebound flare resides afterwards, IgE will gradually decline, repeating fluctuation according to flare development due to exposure to irritants such as allergens, to the level reliable as an AD evolution marker. At this stage, Dr. Cork’s etiology corresponds to clinical experience in steroid withdrawal, the phenomenon called “hypersensitivity after steroid discontinuation.”
I think sharp variation of IgE and eosinophil levels immediately after withdrawal needs explanation considering immune system involvement in addition to skin bariier disruption.
Around 1998 when this paper was written, it was studied how steroids are involved in cytokine production in T cells. Researchers were interested in the strange phenomenon that steroids inhibit synthesis of most cytokines but increase Th2 cytokine, IL-4.
Dr. Rosemarie thought steroids may suppress the production of IL-12, which reduces IL-4 production, to increase IL-4, and proved it with experiments. The above excerpt was quoted from Discussion of her study. Making it simple, steroids seem to suppress inflammation in a short term but inhibit the transition from Th2 to Th1, possibly disturbing the natural healing mechanism.
However this remains controversial and a Swiss doctor expressed a different view in the paper on IL-12 in 2000.
Down-regulation of IL-12 by topical corticosteroids in chronic atopic dermatitis
By N Yawalkar etc. published in the J Allergy Clin Immunol Volume 106, Issue 5, Pages 941-947
He favors steroid application and writes that topical steroids inhibiting IL-12 synthesis prevent atopic dermatitis from proceeding to a chronic stage, where Th1 is predominant.
Such conflicting views come from a different perspective, considering the transition from Th2 (humoral immunity) to Th1 (cellular immunity) inflammation as the process of natural healing or that toward chronicity (obstinacy).
At any rate, Dr. Rosemarie’s concern about steroids that act to suppress IL-12 synthesis seems to have been forgotten since then.
Immune response is a chain of reactions and it is difficult judging whether a certain phenomenon is beneficial or not only by seeing a fraction of it. On the contrary, Dr. Cork’s barrier disruption theory is really clear and easy to understand.
Although the barrier disruption theory is prevalent as an explanation for steroid addiction or rebound, I think Dr. Rosemarie’s concern in 1998 is not groundless.
I have often seen IgE or eosinophil, a part of the immune system, remarkably increase in steroid addictive patients after withdrawal. It was not rare for IgE having kept normal value (within 500) to skyrocket to several tens of thousands or occasionally to hundreds of thousands, or for eosinophil to account for more than 50% of leukocytes in patients undergoing withdrawal (experiencing rebound). I think this phenomenon cannot be explained enough by vulnerability to allergen penetration based on Dr. Cork’s barrier disruption theory. ”Cytokine storm” of IgE or eosinophil version is happening. I think it is necessary to give supplemental explanation with the immune system involved.
The IgE and eosinophil levels, considered as AD severity markers, remain high for a while after steroid withdrawal and are not useful for judging flare conditions. They will go down only when steroids are administered again, which does not mean remission at all. As the rebound flare resides afterwards, IgE will gradually decline, repeating fluctuation according to flare development due to exposure to irritants such as allergens, to the level reliable as an AD evolution marker. At this stage, Dr. Cork’s etiology corresponds to clinical experience in steroid withdrawal, the phenomenon called “hypersensitivity after steroid discontinuation.”
I think sharp variation of IgE and eosinophil levels immediately after withdrawal needs explanation considering immune system involvement in addition to skin bariier disruption.

|

|
