Chapter 18 Experiment by Dr.Kao
Short-Term Glucocorticoid Treatment Compromises Both Permeability Barrier Homeostasis and Stratum Corneum Integrity : Inhibition of Epidermal Lipid Synthesis Accounts for Functional Abnormalities.
By J S Kao et al. published in the J Invest Dermatol 120: 456-464 1523-1747.2003
In 2006, Dr. Cork revealed that topical corticosteroids effectively suppress inflammatory response in the short term and make us feel eczema has been cleared, but in the long run they destroy the skin barrier to make the skin susceptible to irritations, leading to steroid addiction. This theory is supported by the fundamental study conducted by Dr. Kao et al. in 2003.
Short-Term Glucocorticoid Treatment Compromises Both Permeability Barrier Homeostasis and Stratum Corneum Integrity : Inhibition of Epidermal Lipid Synthesis Accounts for Functional Abnormalities.
By J S Kao et al. published in the J Invest Dermatol 120: 456-464 1523-1747.2003
In 2006, Dr. Cork revealed that topical corticosteroids effectively suppress inflammatory response in the short term and make us feel eczema has been cleared, but in the long run they destroy the skin barrier to make the skin susceptible to irritations, leading to steroid addiction. This theory is supported by the fundamental study conducted by Dr. Kao et al. in 2003.
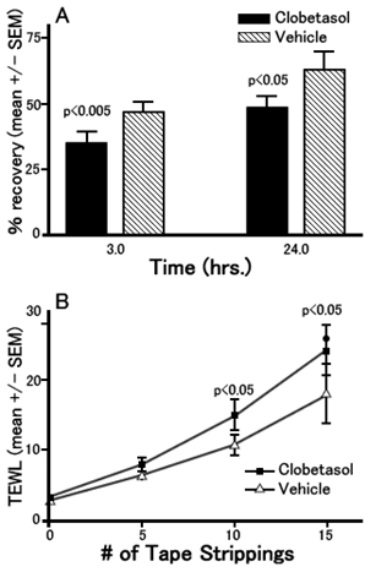
The experiment started with topically applying 0.05% clobetasol (corticosteroid) on the volar forearm of healthy subjects once a day for 3 days to determine TEWL (transepidermal water loss). At this point, the TEWL was almost the same as that of control subjects.
Then, the skin at the above-mentioned site was tape stripped repeatedly. As the adhesive tape peels off corneocyte, repeated tape stripping destroys the epidermal barrier, raising the TEWL. But this is a temporary phenomenon, and the TEWL should recover with the regeneration of corneocyte. Figure A shows the TEWL values measured during this recovery process (3 and 24 hours after the tape stripping). We can see the recovery of clobetasol-applied sites is significantly later than that of non-applied sites.
The more times tape stripping is repeated, the higher the TEWL immediately after tape stripping is conducted. Figure B shows the difference between a topical steroid-applied group and a non-applied group, which gets bigger as tape stripping is repeated more times.
The above results show barrier function impairment due to topical desmosome destruction which begins following only 3 days of topical corticosteroid application.
Then, the skin at the above-mentioned site was tape stripped repeatedly. As the adhesive tape peels off corneocyte, repeated tape stripping destroys the epidermal barrier, raising the TEWL. But this is a temporary phenomenon, and the TEWL should recover with the regeneration of corneocyte. Figure A shows the TEWL values measured during this recovery process (3 and 24 hours after the tape stripping). We can see the recovery of clobetasol-applied sites is significantly later than that of non-applied sites.
The more times tape stripping is repeated, the higher the TEWL immediately after tape stripping is conducted. Figure B shows the difference between a topical steroid-applied group and a non-applied group, which gets bigger as tape stripping is repeated more times.
The above results show barrier function impairment due to topical desmosome destruction which begins following only 3 days of topical corticosteroid application.
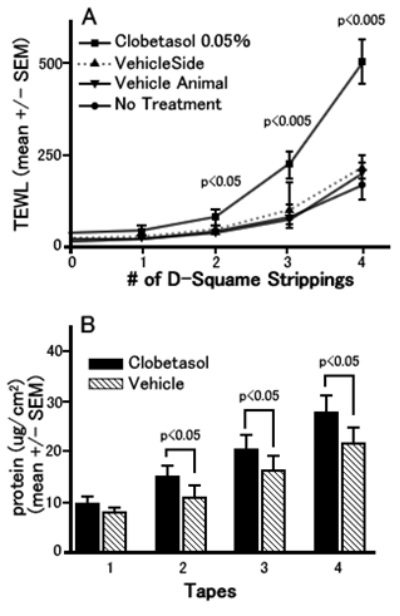
The next experiment was conducted using hairless mice. D-Squame is the name of adhesive tape. Comparison was made among 4 groups: clobetasol was applied to one side of murine flanks for three days (clobetasol 0.05%) and only Vehicle was applied to the other side of flanks of the same mice (vehicle side); Vehicle was applied on both sides of murine flanks (vehicle animal); and nothing was applied (no treatment). In the clobetasol 0.05% group, as tape stripping is repeated, the TEWL gets higher in the larger rate than other groups, which shows the impairment of epidermal barrier function (see Figure A).
Figure B shows the measurements of the amount of protein on the tape strips removed from the mouse skin. The more times tape stripping is repeated, a larger amount of protein is adhered to the tape corresponding to the TEWL increase in Figure A. This indicates that the TEWL increase was led by desmosome destruction that allows corneocytes to be adhered to the tape and removed.
Figure B shows the measurements of the amount of protein on the tape strips removed from the mouse skin. The more times tape stripping is repeated, a larger amount of protein is adhered to the tape corresponding to the TEWL increase in Figure A. This indicates that the TEWL increase was led by desmosome destruction that allows corneocytes to be adhered to the tape and removed.
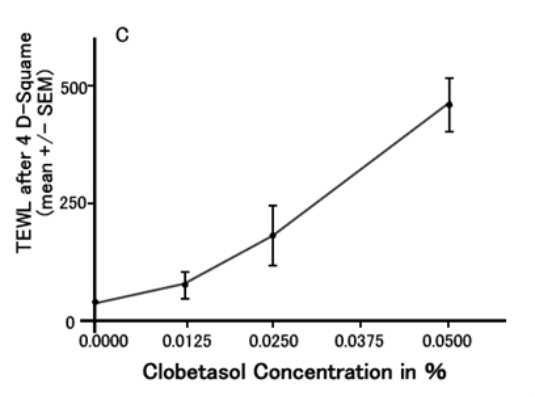
Figure C shows how the TEWL changes according to the clobetasol concentration. This indicates that topical corticosteroids destroy the epidermal barrier in a dose- dependant manner.
Additionally this paper revealed, by means of electron microscopy, that topically applied steroid decreases and weakens corneodesmosomes, and also inhibits lipid synthesis and impairs lamella body formation.
Dr. Kao writes in Discussion as follows.
---- Excerpt -----
It is noteworthy that both psoriasis and atopic dermatitis are associated with defective barrier function and that perturbations in the barrier are already known to initiate or exacerbate these disorders. It is therefore possible that GC treatment induces disease flares in these disorders by further impairing permeability barrier function, and that topical lipid replacement again might ameliorate these flares.
----- End of excerpt -----
Following the above findings, Dr. Cork advocated the mechanism that topical corticosteroids impair the epidermal barrier function, leading to steroid addiction in patients with atopic dermatitis (AD).
What is great with Dr. Cork is that he correctly recognized steroid addiction as a clinician, and logically formulated and simply explained the occurrence mechanism referring to the past study by Dr. Kao at el.
The newest version of the guidelines of care for atopic dermatitis published by the American Academy of Dermatology in 2004 does not refer to steroid addiction. But I predict the next version will note that prolonged use of topical steroids should be avoided to prevent steroid addiction as a side effect and rebound phenomenon after discontinuation in light of Dr. Cork’s epidermal barrier disruption theory having repeatedly been carried by authoritative magazines since 2006.
I guess the number of AD patients suffering from steroid addiction in Japan is far more than that in Europe and the U.S., for topical steroids are available much cheaper than the original price under the national health insurance system. Considering this situation, Japanese dermatological academia should have taken leadership in investigating and reporting on steroid addiction and withdrawal. I can’t help grieving to see some doctors of authority continue to hide the truth and even propagate that steroid addiction is an “unscientific fantasy created by the atopic business.”
Additionally this paper revealed, by means of electron microscopy, that topically applied steroid decreases and weakens corneodesmosomes, and also inhibits lipid synthesis and impairs lamella body formation.
Dr. Kao writes in Discussion as follows.
---- Excerpt -----
It is noteworthy that both psoriasis and atopic dermatitis are associated with defective barrier function and that perturbations in the barrier are already known to initiate or exacerbate these disorders. It is therefore possible that GC treatment induces disease flares in these disorders by further impairing permeability barrier function, and that topical lipid replacement again might ameliorate these flares.
----- End of excerpt -----
Following the above findings, Dr. Cork advocated the mechanism that topical corticosteroids impair the epidermal barrier function, leading to steroid addiction in patients with atopic dermatitis (AD).
What is great with Dr. Cork is that he correctly recognized steroid addiction as a clinician, and logically formulated and simply explained the occurrence mechanism referring to the past study by Dr. Kao at el.
The newest version of the guidelines of care for atopic dermatitis published by the American Academy of Dermatology in 2004 does not refer to steroid addiction. But I predict the next version will note that prolonged use of topical steroids should be avoided to prevent steroid addiction as a side effect and rebound phenomenon after discontinuation in light of Dr. Cork’s epidermal barrier disruption theory having repeatedly been carried by authoritative magazines since 2006.
I guess the number of AD patients suffering from steroid addiction in Japan is far more than that in Europe and the U.S., for topical steroids are available much cheaper than the original price under the national health insurance system. Considering this situation, Japanese dermatological academia should have taken leadership in investigating and reporting on steroid addiction and withdrawal. I can’t help grieving to see some doctors of authority continue to hide the truth and even propagate that steroid addiction is an “unscientific fantasy created by the atopic business.”

|

|
